

CASE OF THE WEEK
2021-41/October 11
Contributors: Levent Trabzonlu, Guliz A. Barkan
A man in his late 20s presented with a left testicular mass found on self-examination. Orchiectomy was performed.



Quiz
1. What is the correct diagnosis?
a. Capillary hemangioma
b. Chronic orchitis
c. Extramedullary hematopoiesis
d. Splenogonadal fusion
e. Testicular lymphoma
2. Which of the following congenital abnormalities could be associated with this entity?
a. Peromelia
b. Encephalocele
c. Gastroschisis
d. Esophageal atresia
e. Club foot
1.d, 2.a
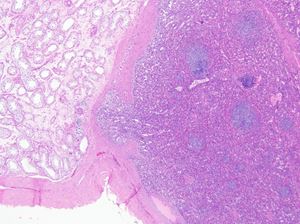
Splenogonadal fusion
A left orchiectomy was performed to reveal a well-defined encapsulated, “beefy” red mass measuring 1.4 x 1.2 x 1.1 cm. Histologic examination of the mass revealed a well-circumscribed mass with a thick fibrous capsule; composed of capillary vessels, sinusoids, and large, thick-walled vessels and interspersed lymphoid follicles. CD34 highlights the endothelial cells and Cd8 highlights the littoral cells. Background testis showed no pathologic abnormality. The patient’s LDH, beta-HCG, and AFP levels were within normal limits. No other congenital abnormalities are present.
Splenogonadal fusion is a rare congenital anomaly in which splenic parenchyma is found in a close proximity of gonadal tissue, first described in1883 by Bostroem.(1) Most cases occur on the left side (98%). The patients are usually young adults or adolescents, with 72% of cases being under 20 years of age. About 57% are associated with other congenital anomalies, including peromelia, micrognathia, and cardiac anomalies. Most cases are discovered incidentally at autopsy or surgery for cryptorchidism or inguinal hernia. The most common presentation is painless scrotal mass. (2,3)
There are two types of splenogonadal fusion: continuous and discontinuous. The continuous type is characterized by the presence of a cord between the orthotopic spleen and the gonad. This cord often comes from the upper pole of the spleen and ends at the upper pole of the gonad. In the discontinuous type, there is no connection between the spleen and the ectopic splenic tissue.(4)
The exact pathogenesis is not yet clear, but it is generally thought to result from early fusion of the spleen and gonad during embryonic development. In the fifth week of gestation, the stomach is moved to the left of the median plane and turns around its axis. This gastric rotation brings together the two spleen and gonad tissues, thus, an event occurring during this period can cause fusion of the surface of the developing genital ridge and the splenic outline. This also accounts for the frequency of left side localization of most cases.(5) The limb buds and mandible develop around the same time, possibly accounting for the association of splenogonadal fusion with peromelia and micrognathia.
Preoperative diagnosis of splenogonadal fusion by radiocolloid spleen scintigraphy has been used, however at smaller centers this technology may not be readily available. Most surgeons select radical treatment to decrease the risk of missing malignancy. Urologist awareness of this entity may enable testis sparing surgery in future cases.
1. Bostroem E. Demonstration eines Praparated von Verwachswung der Mils mit dem lenken Hoden. Gesellschaft deutscher Naturforscher und Aerzte, Verhandlungen der. 1883;56:149.
2. Bostwick DG MJ. Spermatic Cord and Testicular Adnexa. In: Dg CLMG, editor. Urologic Surgical Pathology. Elsevier; 2020. p. 834–53.
3. Alsunbul A, Alsuhaibani S, Al Ali H, Alhussain T, Aldawsari N, Alhathal N. Splenogonadal fusion: A rare case report and literature review. Urol Case Rep. 2020 Nov;33:101307.
4. Putschar WG, Manion WC. Splenicgonadal fusion. Am J Pathol. 1956 Jan;32(1):15–33.
5. Kadouri Y, Carnicelli D, Sayegh HE, Benslimane L, Nouini Y. Pathogenesis, Diagnosis, and Management of Splenogonadal Fusion: A Literature Review. Case Rep Urol. 2020 Oct 7;2020:8876219.
Levent Trabzonlu
Guliz A. Barkan
Loyola University Medical Center
Testis
Splenogonadal fusion, testis, scrotal mass.